Transposition of the great arteries (TGA), also called transposition of the great vessels, is a birth defect involving the two main arteries in the heart being switched. It is a common birth defect, occurring in 5.1 per 10,000 live births, as indicated by the latest Texas Birth Defects Registry research.
The normal heart has four chambers: two upper chambers called atria, which receive blood into the heart, and two lower chambers called ventricles, which pump blood out of the heart. Ordinarily, unoxygenated (blue) blood comes back from the body into the right atrium, moves into the right ventricle, and then is pumped out of the right ventricle through the pulmonary artery (the main artery to the lungs) to collect more oxygen. The now-oxygenated (red) blood returns from the lungs and enters the left atrium, moves into the left ventricle, and then is pumped out to the body through the aorta (the body’s main artery).
With TGA, the pulmonary artery (which normally takes blood from the right side of the heart to the lungs) comes off the left side of the heart and the aorta (which normally takes blood from the left side of the heart to the body) comes off the right side of the heart. Thus, the vessels are said to be “transposed” or “switched.” However, the inflow to each side of the heart is normal. This means that the oxygen-poor (blue) blood from the body enters the heart’s right side and fails to be sent to the lungs to receive oxygen before it is returned to the body. At the same time, oxygen-rich (red) blood from the lungs entering the heart is returned to the lungs through the pulmonary artery, instead of being sent to the body. Thus, babies are not getting enough oxygen for their other organs to function well.
Often, TGA is accompanied by other heart defects, which actually may help infants survive until prompt treatment. These defects include a hole between the heart’s upper chambers (atria), known as an atrial septal defect, or lower chambers (ventricles), known as a ventricular septal defect. Both defects allow blood to mix, enabling some oxygenated blood to get to the body and some unoxygenated blood to get to the lungs. The size of the hole in the heart is sometimes inadequate and needs to be enlarged in newborns by a specially trained cardiologist.
Also boosting oxygen is often an extra blood vessel – patent ductus arteriosus – that joins the heart’s aorta (main artery) and the lung’s pulmonary artery in the womb but usually closes soon after birth, when the infant can breathe air on his or her own.
What Are the Causes?
TGA is a congenital heart defect that occurs as the heart develops during the first eight weeks of pregnancy. In most children, the problem occurs spontaneously, without a known cause. Genes may rarely contribute: If you have a child with a congenital cardiac defect, the chance of having another child with a heart defect is about 2% to 3%. Mothers with Type 1 diabetes also have a slightly higher risk of having babies with TGA. Three of five infants with TGA are boys.
What Are the Symptoms?
Shortly after birth – usually within a week, and at most one month later - a newborn with TGA develops a bluish tint to lips, nails and skin (due to lack of oxygen), as well as rapid or labored breathing, cold, clammy skin, a weak pulse, a pounding heart or a heart murmur – or whooshing sound – heard via stethoscope.
How Is It Diagnosed?
TGA may be diagnosed during pregnancy with a fetal echocardiogram, which is a specialized ultrasound of the fetal heart. The affiliated physicians in the Fetal Cardiology Program at The Fetal Center will confirm a diagnosis and prepare a delivery plan for both mom and baby. A multidisciplinary team of specialists will also develop the baby's immediate care plan following delivery.
If TGA is not diagnosed in utero, and suspicion of a heart defect occurs after the baby is born, a pediatrician will refer the patient to a pediatric cardiologist or neonatologist to determine the diagnosis. The most common tests are:
- Pulse oximetry, a small and painless gadget placed on a finger, which may reveal low oxygen rates from an inefficient heart, sometimes before any other signs of heart distress are apparent.
- Chest X-rays, a painless test that produces images of the heart and lungs, making major flaws visible, such as fluid buildup in the lungs.
- An echocardiogram (ECHO), a painless exam using sound waves to create images of the heart on a computer screen.
- An electrocardiogram (EKG or ECG), a painless exam which checks the heart’s electrical action to reveal irregular rhythms, suggesting a stressed right ventricle.
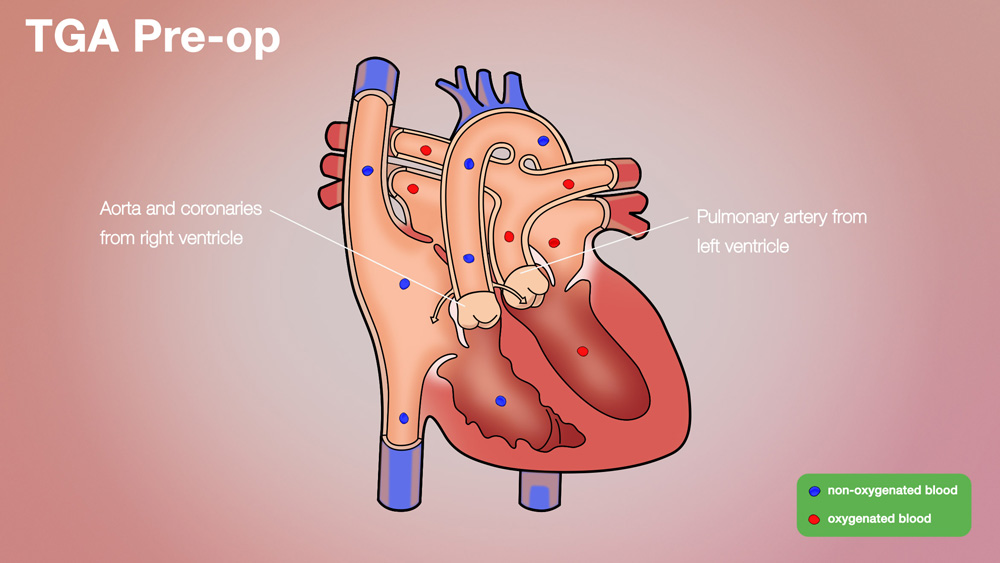
Transposition of the Great Arteries (TGA) Pre-op
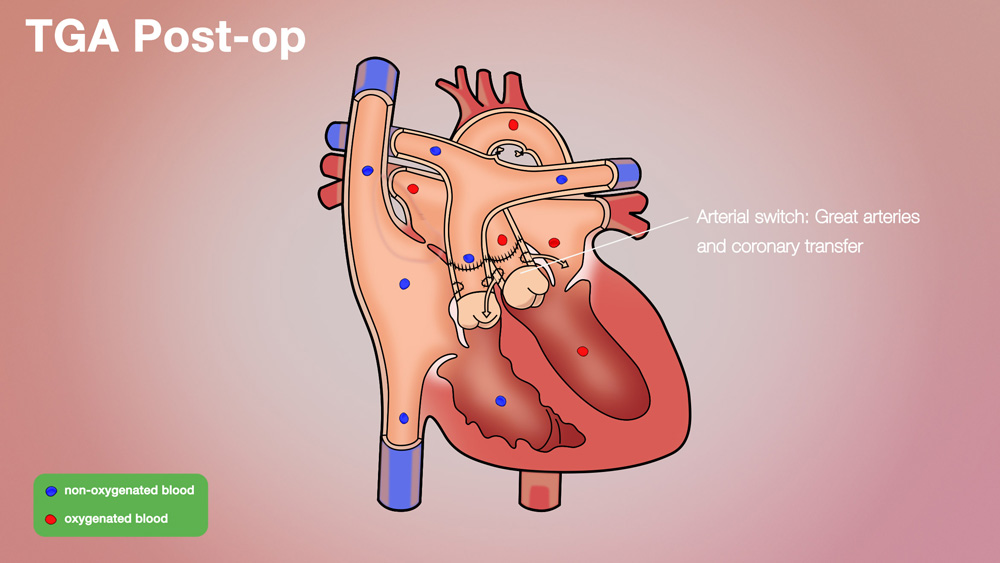
Transposition of the Great Arteries (TGA) Post-op
How Is It Treated?
All children with TGA need surgery called an arterial switch procedure to correct the defect. Prior to surgery, the infant must be stabilized in a way that allows for the red and blue blood to mix. Most babies are started on a medication called prostaglandin (PGE1). This agent is delivered through an IV, keeping the ductus arteriosus (PDA) open. Some babies will also require a balloon atrial septostomy, a procedure in which a balloon, inserted through a vein in the groin or belly button, is used to enlarge a small hole between the upper chambers of the heart. This also allows for better mixing of red and blue blood.
In an arterial switch procedure, the main pulmonary artery and the aorta are divided above the heart, their positions are reversed (or switched), and then they are sewn in place on the correct side. The switching of the pulmonary artery and aorta is usually accomplished without difficulty. The more delicate and highly technical part of the arterial switch is the moving of the coronary arteries. The coronary arteries are small arteries that supply the heart muscle itself with blood. They come off the aorta below where the aorta is “switched,” so the coronaries must be switched separately. Transferring the coronary arteries to their new home can be tricky, because the vessels are small and may become occluded in the process. To make matters worse, nearly one-third of all patients with TGA have an unusual branching pattern of their coronary arteries. Some of those branching patterns make the transfer of the coronary arteries much more difficult.
Surgery for TGA is usually done within the first two weeks of life. Even though most children do very well with the operation, it still represents major open heart surgery on a newborn. Most babies will spend several days in the intensive care unit after surgery and many will spend longer. The majority of babies will spend an additional 1-3 three weeks in the hospital.
After surgery, the child may need medication to help his or her heart pump efficiently and control heartbeat and blood pressure while limiting excess fluid in the body. Rarely, a pacemaker may be needed to help the heart beat normally.
What Are the Long-Term Effects?
For most children with TGA, the prognosis is excellent. If an arterial switch is successful, there is a good chance that a child may be expected to live an entirely normal life, both in terms of longevity and activity level. However, it cannot be overstated that in TGA there is often a great deal of difference between individual patients. One must keep these differences in mind when evaluating children.
What Follow-Up Care Is Needed?
Parents will help with wound care as the baby heals post-surgery. The child’s cardiologist will monitor for leaky valves, irregular heartbeat, narrowed blood vessels at surgical sites or other heart issues that may arise later in life.
Why Choose the Children’s Heart Institute?
At Children’s Heart Institute at Children’s Memorial Hermann Hospital, patients with congenital or acquired heart disorders receive hands-on specialized care 24/7 from a team of affiliated physicians and specialty-trained nurses who aim to deliver the best possible outcomes.
Children’s Memorial Hermann Hospital was named one of the top children's hospitals nationally in Cardiology & Heart Surgery by U.S. News & World Report. In addition, Children’s Heart Institute is among the top congenital heart surgery programs in North America for patient care and outcomes, according to the Fall 2019 Society of Thoracic Surgeons (STS) Congenital Heart Surgery Database Report of 118 STS participating programs.
In collaboration with various subspecialties, the affiliated team provides comprehensive care for newborns, children and adolescents, with the ability to transition into adult congenital cardiac care. Team members have the experience and skills necessary to offer innovative treatment methods and specialized services, including, but not limited to:
- Biventricular repairs and biventricular conversions
- Congenital heart optimization
- Full repairs for complex congenital heart defects in newborns
- Hybrid catheterization and surgical procedures
- Minimally invasive transcatheter pulmonary valve (TPV) therapy
- Minimally invasive repairs
- Treatment for adult congenital heart disease
- Valve repairs and preservation
With the Level IV Neonatal Intensive Care Unit (NICU) and a dedicated Children’s Heart Institute Intensive Care Unit at Children’s Memorial Hermann Hospital, critical heart patients have access to quality, specialized care. By utilizing state-of-the-art techniques, the team at Children’s Heart Institute strives to offer patients with the most complex problems the greatest opportunity for a normal life.
Contact Us
If you have any questions, use the online tool below to help us connect with you. To refer a patient or schedule an appointment, please contact our clinic using the information below.
- Pediatric Cardiology Clinic
The University of Texas Health Science Center Professional Building
6410 Fannin, Suite 370
Houston, TX 77030
Phone: (713) 486-6755 (Appointment Line)
- Pediatric and Congenital Heart Surgery Clinic
The University of Texas Health Science Center Professional Building
6410 Fannin, Suite 370
Houston, TX 77030
Phone: (713) 500-5746
CMHH-Heart@memorialhermann.org
To contact Children’s Heart Institute at Children’s Memorial Hermann Hospital, please fill out the form below.
The Children’s Heart Institute is a collaboration between the affiliated physicians at McGovern Medical School at UTHealth Houston and Children’s Memorial Hermann Hospital. Typically, patients are seen on an outpatient basis at a UT Physicians clinic with all inpatient procedures performed at Children’s Memorial Hermann Hospital.
Nationally Ranked Pediatric Care
Proud to be named one of the nation’s best in Cardiology and Heart Surgery; Gastroenterology and GI Surgery; Neonatology; and Neurology and Neurosurgery.
Learn More